Hospital lights and environmental disinfectants In Damavand ( Sale, implementation consultation )



You can introduce your business services or products in this section.
For this purpose, be in touch with us.
Although the dose measurement system used in our study (FastCheck Mediland, Taoyuan City , Taiwan) is semi-quantitative, it allowed us to detect if the dose reached adequate values for disinfection and to repeat the application when the value was not satisfactory. However, each dose value exceeded the expected value. This demonstrates that the device was positioned correctly in order to avoid shadow areas, although it was necessary to properly place furniture and equipment to improve the irradiation of all surfaces. In the study conducted by Wong et al., the R-D Rapid Disinfector system (Steriliz, Rochester, NY, USA) was used in a tertiary care hospital to evaluate the incremental benefit of UV-C disinfection in isolation rooms after the discharge of infected patients. The employed robot used four detached sensors to directly measure the UV-C light [
In our study, we evaluated the efficacy of the UV-C treatment only on the reduction in mesophilic growth that mainly represents human contamination, but not on specific pathogens of interest; however, the reduction was very significant, suggesting that this system can easily eliminate pathogens as well. We have previously demonstrated that the adoption of an automated UV-C-disinfection robot in the enhancement of SOP in high-risk settings was successful in reducing pathogens on high-touch surfaces, improving the patient&#x;s safety [
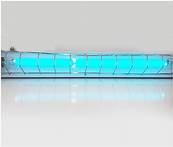
The UV-C disinfection robot (Mediland Enterprise Corporation, Taoyuan City, Taiwan) uses amalgam lamps (UV lamp NNI / XL Niederdruck VUV Strahler) and protective reflector technology to generate high-energy, broad-spectrum ultraviolet light (UV-C &#x; nm). The manufacturer of the lamps declares in the technical data sheet that the lamps have a filter that blocks radiation between &#x; nm, eliminating the possibility of producing ozone as a by-product of UV-C radiation. The UV-C device uses min disinfection cycles and multiple positions with minimal distances from high-touch surfaces. Due to the use of high-intensity UV-C radiation, the device must operate in unoccupied rooms. There are multi-motion sensors that shut off the device if any movement is detected inside the room being disinfected or if the door is accidentally opened. When the robot operates in accordance with these procedures, the manufacturer declares that the amalgam lamps produce no ozone gas and leave no toxic residues.
Moreover, it would be important to evaluate the advantages of implemented cleaning and disinfection protocols with the use of UV-C devices in areas hosting fragile and vulnerable patients, e.g., in intensive care units. The principal limitation is the continuous presence of people in this type of setting. For this reason, it would be worth evaluating strategies aimed at protecting the patient&#x;s safety using protective devices, which may be evaluated for human security during UV-C emission at specific dosages and times.
The cleaning procedure is not only dependent on the chemicals used but also on the personnel performing it. As reported by Toffollutti et al., there are differences between housekeeping and outsourcing cleaning staff in ensuring adequate levels of hygiene; outsourcing cleaning services was associated with a greater incidence of meticillin-resistant Staphylococcus aureus (MRSA) and worse patient perceptions of cleanliness [